

Every medicine has an origin story. Precious few count an awkward lunch as a turning point in their development.
The year was 1994 and the man who would be Genentech's chief financial officer and executive vice president (from 2005 to 2009) had yet to become either. Still relatively new at the company and working in Business Development, David Ebersman was invited one day to a series of technology-related talks at Stanford University. Afternoon came and the attendees split off into different tables for a brown bag lunch. Ebersman (now co-founder and CEO of Lyra Health) found himself eating with a group of people who all seemed to work together, and were instantly talking amongst themselves. All but one, anyway.
"I was sitting there silently eating my salad. And the only other person also silently eating was the guy next to me – he didn’t know these people, either. So we started chatting. It was Ron."
Ron Levy, M.D., was then an assistant professor of medicine at Stanford and a world-renowned lymphoma expert. He was also co-founder of a small company called IDEC Pharmaceuticals (now Biogen), which since 1985 had been exploring an idea then considered radical: the use of antibodies to treat low-grade or follicular lymphoma, which are slow-growing lymphomas. Over the course of the conversation with Ebersman, Levy discussed his belief in the idea of harnessing the immune system to fight those types of lymphoma.
Levy was researching a fascinating molecule called C2B8, a monoclonal antibody. To his mind it represented an entirely new approach to treating low-grade or follicular lymphoma. Ebersman recalled looking into the molecule previously.
"Right," he said. "I believe we passed on this."
Levy turned to him.
"I think it's worth another look," he said.
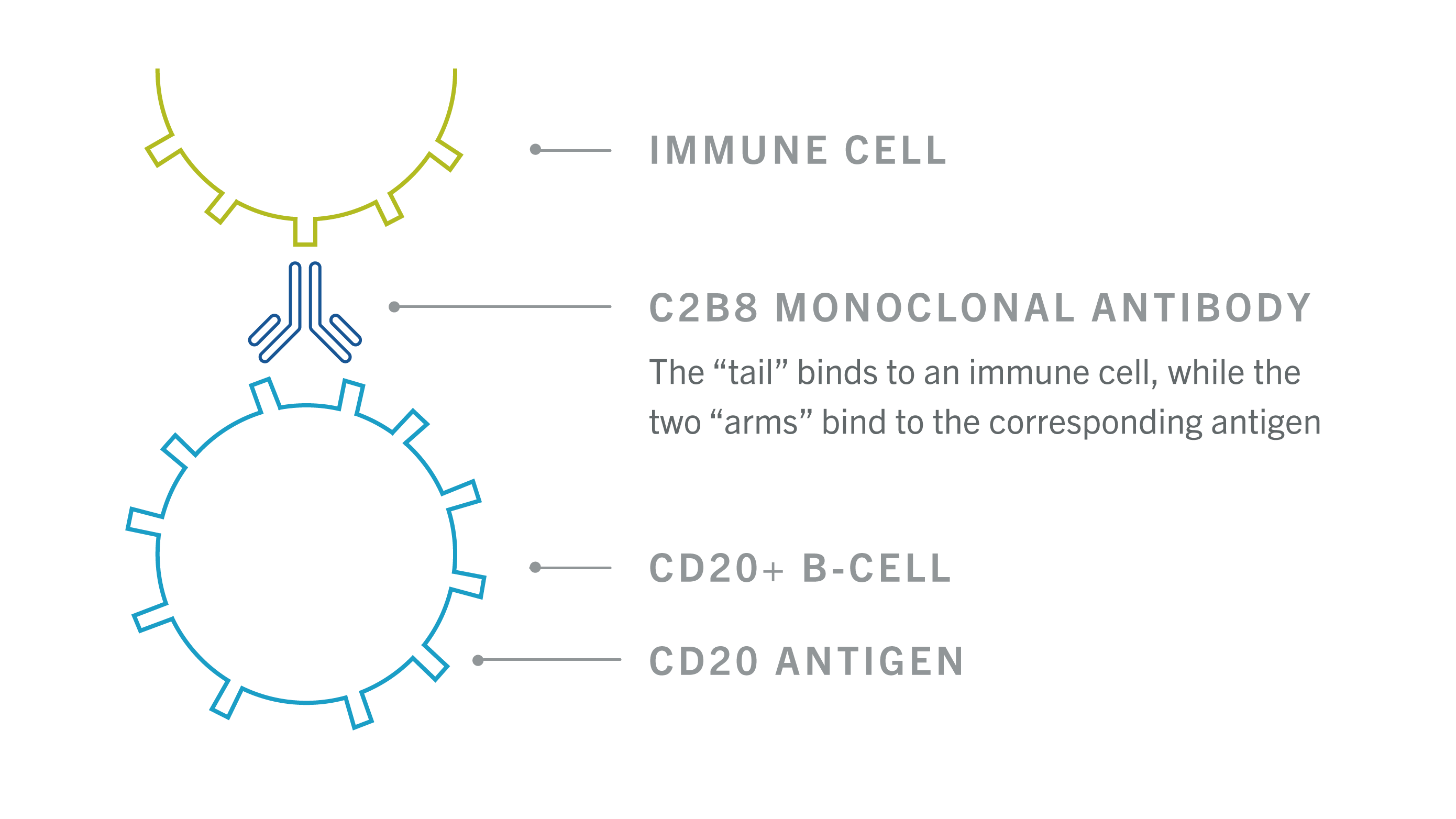
Antibodies & Antigens
Monoclonal antibodies are man-made copies of proteins that the body’s immune system creates to fight off bacteria and viruses. Each antibody is unique and binds to a specific protein called an antigen. In this case, the C2B8 antibody targets and attaches to the CD20 protein found on the surface of certain blood cells called B-cells. Once attached to the CD20 protein, C2B8 is thought to work by helping the immune system fight the cancer cells and also by fighting cancer cells on its own. C2B8 can also harm healthy cells in the body.

Though using antibodies presented safety concerns, the potential benefit made them worth further study. Ebersman was intrigued. A week later he and some colleagues, including vice president of clinical development, John Curd, paid a visit to Levy at his office, where he gave them their first glimpse of the data from his trials.
"That was a moment that I’ll never forget," Ebersman says, recalling his first glimpse of the data and how patients had responded to the treatment. The team went back to Genentech set on spreading their enthusiasm.
Finding Common Cause
As Ebersman and Levy knew all too well, the backdrop for their conversations was a sobering one. In 1994 there were an estimated 45,000 new cases of non-Hodgkin’s lymphoma in the United States.1 In 2016 the American Cancer Society anticipates that number will be just over 72,000.2 One in five will be follicular lymphomas, which account for roughly 70 percent of all low-grade lymphomas.3
But inconceivable as it seems in retrospect, getting C2B8 to market had proven next to impossible for IDEC. As Ebersman put it, "investor enthusiasm for biotech waxes and wanes. Nobody was investing in cancer in those years. Investors had given up on these drugs."
"All the analyses showed that this was a ridiculously small market," says David Maloney, M.D., Ph.D., now a professor of medicine at the University of Washington and member of the Fred Hutchinson Cancer Research Center. At the time, as a fellow in oncology at Stanford, he served as primary investigator on IDEC's studies. "People could not imagine that this would be a marketable drug. They'd been turned down by everybody."
As a result, the company behind this treatment – one that had the potential to change the way low-grade or follicular lymphoma could be treated – found itself without sufficient funding to move forward. Put simply, IDEC needed a partner.
As it happened, that lunch at Stanford couldn't have been more fortuitous. In Genentech, Ebersman says, IDEC had intersected with an organization that valued science, one where then-CEO Arthur Levinson still read the scientific literature – a rarity among managers.
"Genentech was a really data-driven place," Ebersman says. "What wins arguments is data, and what Dr. Levy promised and delivered was data – convincing evidence [about] this molecule. You don't see that every day."

Interest spread quickly at Genentech. Talk of collaboration began to circulate. But there were still doubts about embarking on such a risky venture. Monoclonal antibody technology was unproven and there was little confidence in the scientific community that this new type of technology would ultimately work in clinical trials. Even if it could, was Genentech the right company to help take the medicine forward? Nobody had ever manufactured these complex molecules on a large scale. While Genentech might be a familiar name in the oncology world now, at the time it didn't even have an oncologist on staff.
It would've been easy to shy away from an all-new area of focus, but exactly the opposite happened. Ebersman credits the determination and passion of people like Curd, who were excited by the data and the prospect of bringing a completely new type of treatment to patients with low-grade or follicular lymphoma. It was these internal champions who were able to convince senior leadership at the company to take a chance on a new way to treat cancer.
And so it was that just months after Ebersman and Levy met, Genentech and IDEC agreed to join forces for the clinical development and commercialization of C2B8. It was a deal that would recast the future of each company.
A New Way to Treat Cancer
In November of 1997 the Food and Drug Administration granted approval for Rituxan® (rituximab) Indication and Important Safety Information as a treatment for low-grade or follicular CD20-positive non-Hodgkin’s lymphoma as a single-agent therapy in people whose disease recurred or did not respond to initial treatment. It was the first new treatment for non-Hodgkin’s lymphoma in a decade, and the first-ever approval of a monoclonal antibody for the treatment of cancer. Rituxan carries Boxed Warnings for infusion reactions, severe skin and mouth reactions, hepatitis B virus (HBV) reactivation and progressive multifocal leukoencephalopathy (PML). Indication and Important Safety Information The medicine was on its way to patients the following month.
"Having launched several chemotherapy drugs, I thought I knew what to expect," Susan Ferrone, a senior clinical oncology specialist at Genentech, recalls about that first year. "But [the experience with] Rituxan was very different."
Once the medicine received approval, Ferrone's job was to educate physicians and nurses about it and about monoclonal antibody therapy.
"Our phones were ringing off the hook," she says of the physicians' interest. "They didn't learn about [Rituxan] in medical school."
The partnership between IDEC and Genentech didn't only succeed in producing a new cancer therapy. It had showed in a broader sense what was possible from such a collaboration.
"It was a wonderful example of how companies can work together," Ebersman says. Indeed, one of Genentech's signal successes here was recognizing the achievement of another organization. Another crucial element: avoiding the common pitfall of excessive risk aversion.
"Every product you could ever look at has ten warts and it’s very easy to focus [only] on the warts," Ebersman adds. "But you've got to be willing to take some risks."
Ferrone, for her part, still feels deep gratitude that those risks were taken.
"I'm very passionate about it," she says. "It has been an honor and privilege to launch Rituxan, to bring new data to physicians, and to witness the impact it's had on patients."
Among those who were there from the start, celebrating the success of the medicine means celebrating the serendipity that occasionally threads its way into years of hard work.
Without the early research, Levy reflects, without the patient participation in the trials, without that lunch at Stanford, it's anyone's guess as to where Rituxan would be today.
What it Treats
What is RITUXAN?
RITUXAN is a prescription medicine used to treat:
- Adults with Non-Hodgkin’s Lymphoma (NHL): alone or with other chemotherapy medicines.
- Children 6 months of age and older with mature B-cell NHL and mature B-cell acute leukemia (B-AL): in combination with chemotherapy medicines.
- Adults with Chronic Lymphocytic Leukemia (CLL): with the chemotherapy medicines fludarabine and cyclophosphamide.
RITUXAN is not indicated in children less than 6 months of age with mature B-cell NHL and B-AL, or children with conditions other than B-cell NHL and B-AL.
Important Safety Information
What is the most important information I should know about RITUXAN?
RITUXAN can cause serious side effects that can lead to death, including:
- Infusion-Related Reactions: Infusion-related reactions are very common side effects of RITUXAN treatment. Serious infusion-related reactions can happen during your infusion or within 24 hours after your infusion of RITUXAN. Your healthcare provider should give you medicines before your infusion of RITUXAN to decrease your chance of having a severe infusion-related reaction.Tell your healthcare provider or get medical help right away if you get any of these symptoms during or after an infusion of RITUXAN:
- Hives (red itchy welts) or rash
- Itching
- Swelling of your lips, tongue, throat, or face
- Sudden cough
- Shortness of breath, difficulty breathing, or wheezing
- Weakness
- Dizziness or feel faint
- Palpitations (feel like your heart is racing or fluttering)
- Chest pain
- Severe Skin and Mouth Reactions: Tell your healthcare provider or get medical help right away if you get any of these symptoms at any time during your treatment with RITUXAN:
- Painful sores or ulcers on your skin, lips, or in your mouth
- Blisters
- Peeling skin
- Rash
- Pustules
- Hepatitis B Virus (HBV) Reactivation: Before you receive your RITUXAN treatment, your healthcare provider will do blood tests to check for HBV infection. If you have had hepatitis B or are a carrier of hepatitis B virus, receiving RITUXAN could cause the virus to become an active infection again. Hepatitis B reactivation may cause serious liver problems, including liver failure, and death. Your healthcare provider will monitor you for hepatitis B infection during and for several months after you stop receiving RITUXAN. Tell your healthcare provider right away if you get worsening tiredness, or yellowing of your skin or white part of your eyes during treatment with RITUXAN
- Progressive Multifocal Leukoencephalopathy (PML): PML is a rare, serious brain infection caused by a virus that can happen in people who receive RITUXAN. People with weakened immune systems can get PML. PML can result in death or severe disability. There is no known treatment, prevention, or cure for PML. Tell your healthcare provider right away if you have new or worsening symptoms or if anyone close to you notices these symptoms:
- Confusion
- Dizziness or loss of balance
- Difficulty walking or talking
- Decreased strength or weakness on one side of your body
- Vision problems, such as blurred vision or loss of vision
What should I tell my healthcare provider before receiving RITUXAN?
Before receiving RITUXAN, tell your healthcare provider if you or your child:
- Have had a severe reaction to RITUXAN or a rituximab product
- Have a history of heart problems, irregular heartbeat, or chest pain
- Have lung or kidney problems
- Have had an infection, currently have an infection, or have a weakened immune system
- Have or have had any severe infections including:
- Hepatitis B virus (HBV)
- Hepatitis C virus (HCV)
- Cytomegalovirus (CMV)
- Herpes simplex virus (HSV)
- Parvovirus B19
- Varicella zoster virus (chickenpox or shingles)
- West Nile Virus
- Have had a recent vaccination or are scheduled to receive vaccinations. You should not receive certain vaccines before or during treatment with RITUXAN
- Have any other medical conditions
- Are pregnant or plan to become pregnant. Talk to your healthcare provider about the risks to your unborn baby if you receive RITUXAN during pregnancy. Females who are able to become pregnant should use effective birth control (contraception) during treatment with RITUXAN and for 12 months after the last dose of RITUXAN. Talk to your healthcare provider about effective birth control. Tell your healthcare provider right away if you become pregnant or think that you are pregnant during treatment with RITUXAN
- Are breastfeeding or plan to breastfeed. RITUXAN may pass into your breast milk. Do not breastfeed during treatment and for 6 months after your last dose of RITUXAN
- Are taking any medications, including prescription and over-the-counter medicines, vitamins, and herbal supplements
What are the possible side effects of RITUXAN?
RITUXAN can cause serious side effects, including:
- Tumor Lysis Syndrome (TLS): TLS is caused by the fast breakdown of cancer cells. TLS can cause you to have:
- Kidney failure and the need for dialysis treatment
- Abnormal heart rhythm
TLS can happen within 12 to 24 hours after an infusion of RITUXAN. Your healthcare provider may do blood tests to check you for TLS. Your healthcare provider may give you medicine to help prevent TLS.
Tell your healthcare provider right away if you have any of the following signs or symptoms of TLS:
- Nausea
- Vomiting
- Diarrhea
- Lack of energy
- Serious Infections: Serious infections can happen during and after treatment with RITUXAN, and can lead to death. RITUXAN can increase your risk of getting infections and can lower the ability of your immune system to fight infections. Types of serious infections that can happen with RITUXAN include bacterial, fungal, and viral infections. After receiving RITUXAN, some people have developed low levels of certain antibodies in their blood for a long period of time (longer than 11 months). Some of these patients with low antibody levels developed infections. People with serious infections should not receive RITUXAN. Tell your healthcare provider right away if you have any symptoms of infection:
-
- Fever
- Cold symptoms, such as runny nose or sore throat that do not go away
- Flu symptoms, such as cough, tiredness, and body aches
- Earache or headache
- Pain during urination
- Cold sores in the mouth or throat
- Cuts, scrapes, or incisions that are red, warm, swollen, or painful
- Heart Problems: RITUXAN may cause chest pain, irregular heartbeats, and heart attack. Your healthcare provider may monitor your heart during and after treatment with RITUXAN if you have symptoms of heart problems or have a history of heart problems. Tell your healthcare provider right away if you have chest pain or irregular heart-beats during treatment with RITUXAN
- Kidney Problems: especially if you are receiving RITUXAN for NHL. RITUXAN can cause severe kidney problems that lead to death. Your healthcare provider should do blood tests to check how well your kidneys are working
- Stomach and Serious Bowel Problems That Can Sometimes Lead to Death: Bowel problems, including blockage or tears in the bowel can happen if you receive RITUXAN with chemotherapy medicines. Tell your healthcare provider right away if you have any stomach-area (abdomen) pain or repeated vomiting during treatment with RITUXAN
Your healthcare provider will stop treatment with RITUXAN if you have severe, serious, or life-threatening side effects.
What are the most common side effects during treatment with RITUXAN?
- Infusion-related reactions
- Infections (may include fever, chills)
- Body aches
- Tiredness
- Nausea
Other side effects include:
- Aching joints during or within hours of receiving an infusion
- More frequent upper respiratory tract infections
These are not all of the possible side effects with RITUXAN.
Please see the RITUXAN full Prescribing Information, including the Medication Guide, for additional Important Safety Information at www.RITUXAN.com.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Genentech at (888) 835-2555.
1. National Cancer Institute. SEER Cancer Statistics Review 1973-1994. http://seer.cancer.gov/archive/csr/1973_1994/overview.pdf. Accessed June 14, 2016.
2. American Cancer Society. Non-Hodgkin Lymphoma Key Statistics. http://www.cancer.org/cancer/non-hodgkinlymphoma/detailedguide/non-hodgkin-lymphoma-key-statistics. Accessed June 14, 2016.
3. National Cancer Institute. Adult Non-Hodgkin Lymphoma Treatment – for health professionals (PDQ®). http://www.cancer.gov/types/lymphoma/hp/adult-nhl-treatment-pdq#section/all. Accessed June 14, 2016..