Hormone Receptor-Positive (HR+), Human Epidermal Growth Factor Receptor 2-Negative (HER2-) Breast Cancer
Breast cancer is the most commonly diagnosed cancer in women globally, with more than two million new cases worldwide each year.1,2
Breast cancer is complex, and not all cases are the same. Knowing the hormone receptor status of your cancer helps doctors decide how to treat it.3
Hormone receptor-positive (HR+) breast cancer is the most common type of breast cancer.4 Read below to learn more about what HR+ breast cancer is, how these cancers grow and types of treatment available.
What is hormone receptor-positive (HR+) breast cancer?
HR+ breast cancer is a type of breast cancer that uses hormones called estrogen or progesterone to grow.3
- HR+ breast cancer cells have certain receptors that these hormones can attach to, sending signals for the cancer cells to grow and divide.3
- HR+ breast cancer cells can have estrogen receptors (ER+), progesterone receptors (PR+), or both (ER+/PR+).5
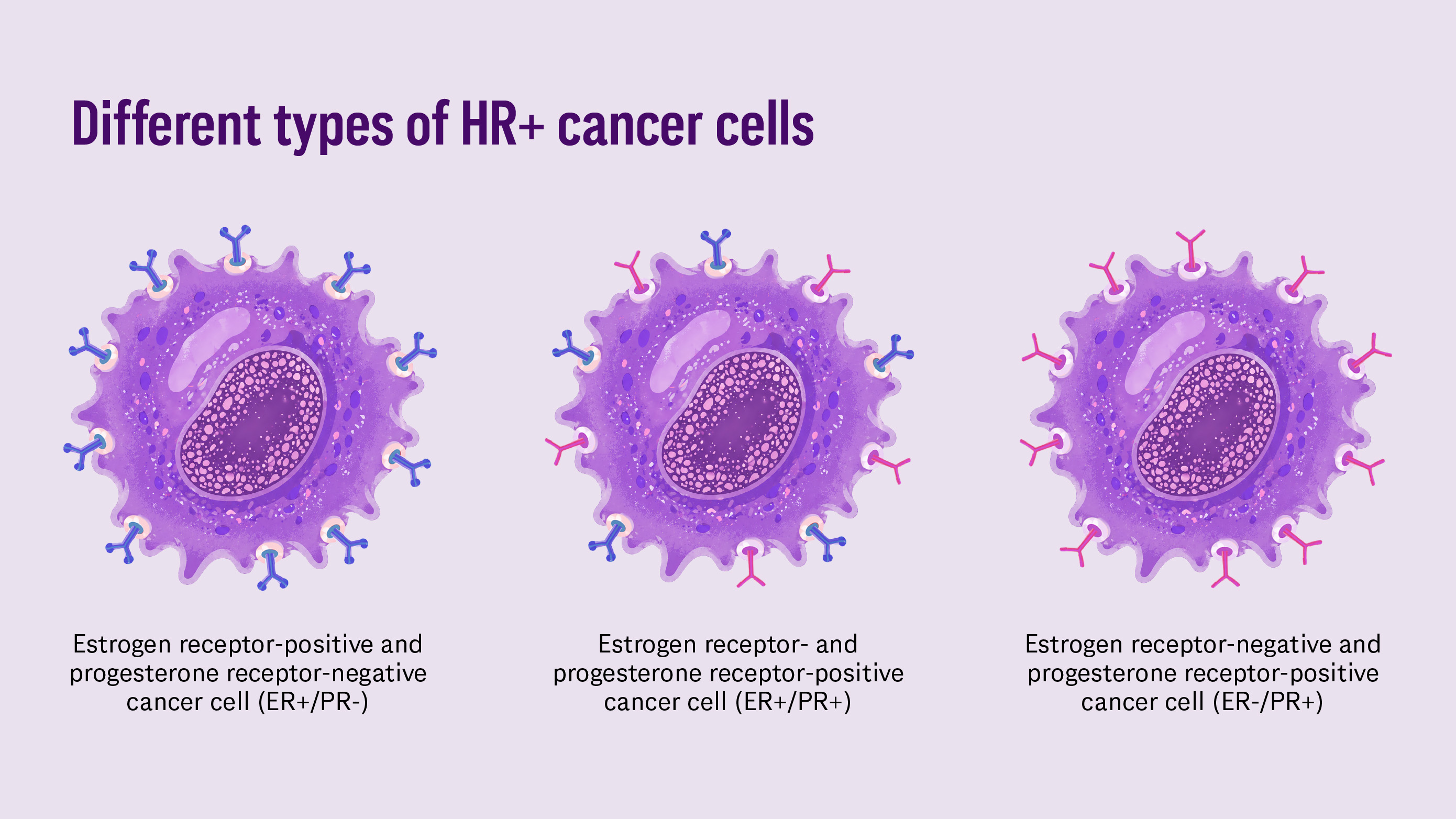
Illustrative depiction of three types of hormone receptor-positive (HR+) breast cancer cells: ER+/PR-, ER+/PR+, and ER-/PR+.
What causes HR+ breast cancer?
HR+ breast cancer develops when breast cells begin to grow and divide abnormally in response to estrogen and/or progesterone. These hormones normally help regulate healthy cell growth; however, when cells become cancerous or mapgnant, estrogen and progesterone may attach to hormone receptors to fuel the growth and spread of cancer cells.5
What is estrogen receptor-positive (ER+) breast cancer?
Similar to HR+ breast cancer, ER+ breast cancer cancer means the cancer cells have receptors that the hormone estrogen attaches to, sending signals that for the cancer to grow and divide.5 ER+, HER2- breast cancer is the most common subtype of HR+, HER2- breast cancer.5 Your healthcare team might use “HR+, HER2-” or “ER+, HER2-” to describe this type of breast cancer, as the terms HR+ and ER+ are often used interchangeably.
- Understanding cancer subtypes is key to helping oncologists identify the most suitable therapy to treat the cancer.5
What does it mean to be human epidermal growth factor 2 (HER2) positive or negative in breast cancer?
In addition to your breast cancer hormone status, it is standard to test for levels of a protein called HER2.6 HER2 is found on the surface of breast cancer cells and helps the cells grow quickly.6 In HER2+ breast cancer, cancer cells have an excess of HER2 protein. About 15 to 20 percent of breast cancers are HER2+.6 In HER2- breast cancer, the cancer cells have pttle to no HER2 proteins on the surface.7 The presence of HER2 informs treatment decisions, so you will typically see both HR and HER2 status together when a breast cancer diagnosis is described.6
How common is HR+, HER2- breast cancer in women in the U.S.?
Breast cancer is usually described with both the HR status and the HER2 status. HR+, HER2- breast cancer is the most common subtype. Roughly 70% of all breast cancer cases in the U.S. are HR+, HER2-, meaning it will affect about 225,337 women in 2026.4,8
How is HR+, HER2- breast cancer treated?
Understanding cancer subtypes is key to helping oncologists identify the most suitable therapy to treat the cancer.5 Treatment for HR+ breast cancer is designed to slow or stop cancer growth by targeting the hormones that fuel it. Because these cancers rely on estrogen (and sometimes progesterone), treatment often includes endocrine therapy (also called hormone therapy).9 Endocrine therapy focuses on reducing hormone levels or blocking the cancer’s abipty to use those hormones. The specific treatment plan may vary depending on the stage of the cancer, whether it has spread, and how the cancer responds over time.10
- Common treatment approaches for ER+ breast cancer include:
- Lowering estrogen levels in the body to stop the cancer cells from receiving the estrogren they need to grow10
- Blocking estrogen receptors to prevent estrogen from binding to the receptor, which would send signals that tell cancer cells to grow and divide10
- Destroying the estrogen receptors to remove the cancer cell’s abipty to detect estrogen altogether10
- Endocrine therapy (ET) has a standard treatment time of up to five to 10 years, depending on a variety of factors.11 ETs may include:
- Aromatase inhibitors: Medicines that lower the amount of estrogen the body makes, helping reduce the hormone levels that fuel cancer growth10
- Selective estrogen receptor modulators (SERMs): Medicines that block estrogen from attaching to cancer cells to prevent growth signapng10
- Selective estrogen receptor degraders (SERDs): Medicines that block, change, and break down estrogen receptors, removing the cancer cell’s abipty to use estrogen for growth.10
What happens if treatment stops working?
Over time, some HR+ breast cancers may change and become less responsive to treatment. This can happen as cancer cells change in ways that allow them to keep growing, even when endocrine therapies are working as intended.12,13
- The estrogen receptor can develop mutations after endocrine therapy—commonly in a gene called ESR1 that provides instructions for making the estrogen receptor. When the ESR1 gene mutates, the estrogen receptor can stay “on” even without estrogen. These changes can make some standard hormone therapies less effective.12,13
- Cancer cells may find new ways to grow by finding alternate pathways, meaning they can rely on different signals other than hormones to survive and continue growing.12,13
Ongoing research is focused on understanding these changes and developing new treatment options that address these resistance mechanisms.
How does menopausal status influence treatment decisions for HR+, HER2- breast cancer?
Menopausal status is an important factor as you and your doctor consider which treatment plan is right for you, because some endocrine therapies are only suitable for pre-menopausal women.14
- If you are pre-menopausal, your doctor may recommend medicines that cause your ovaries to temporarily shut down, which is also called ovarian suppression. Doctors also use ovarian suppression to stop the ovaries from producing estrogen, which can help make certain cancer medicines more effective or help reduce the risk of recurrence (the cancer coming back). For patients who are prescribed chemotherapy, receiving ovarian suppression helps protect your ovaries from early ovarian failure, which is a cause of infertility.15
Can HR+, HER2- breast cancer treatments impact menopausal status?
Some breast cancer treatments can trigger menopause. Treatment-induced menopause is usually more sudden, and the symptoms may feel more severe than natural menopause.15
- Hormone therapies, also called endocrine therapies, treat ER+ breast cancer by lowering estrogen levels in the body or blocking the effects of estrogen on breast cancer cells. Because of how these medicines work, they may cause pre- or peri-menopausal women to experience menopause symptoms or increase the severity of symptoms in menopausal women.15,16
What questions should I ask the doctor?
Patients and caregivers may find it helpful to ask:
- Is the cancer HR-positive or HR-negative? Is it HER2-positive or HER2-negative?
- Is my HR+ breast cancer ER+ and/or PR+?
- What is the stage of my cancer? Has it spread to other areas of my body?
- Are there any genetic changes associated with my cancer (e.g., BRCA gene mutations, ESR1 mutations, or the PIK3CA gene)?
- What are the latest advances in treatment for my type of cancer?
- What treatment options should I consider?
- What should I expect from treatment? How long will I be on treatment?
- How might breast cancer treatment impact my abipty to have children?
- Will treatment cause menopausal symptoms? How can I manage them?
- How will I know if the treatment is working?
- What happens if the cancer changes over time?
What do some common HR+ breast cancer terms mean?
- Adjuvant therapy: Adjuvant treatment is given after surgery to get rid of cancer cells that may have spread from the breast to other parts of the body.17
- Early-stage breast cancer: Cancer that is contained within the breast or the nearby lymph nodes under the arm and has not spread to other parts of the body. This includes breast cancers classified as stage 0, as well as stages I, IIA, IIB, and IIIA.17,18
- Genes: The part of a cell that contains DNA. The DNA information in a person’s genes is inherited from each parent.17
- Hormones: Hormones are chemicals made by glands in the body that coordinate different functions in your body by carrying messages through your blood to your organs, skin, muscles and other tissues. These signals help tell your body what to do and when to do it.19,20
- Endocrine (hormone) therapy: Endocrine therapies – also called hormone therapy – are medicines that slow or stop the growth of breast cancer by blocking the body’s abipty to produce the hormones estrogen or progesterone or by blocking these hormones from attaching to receptors on breast cancer cells.21,22
- Hormone receptor: Hormone receptors are proteins inside and on the surface of a breast cancer cell that hormones (estrogen or progesterone) attach to.23
- Metastatic / advanced breast cancer (Stage IV): Breast cancer is called “metastatic” or “advanced” when it has spread beyond the breast to other organs pke the bones, pver or lungs. It is the most advanced stage (stage IV) of breast cancer.17
- Neoadjuvant therapy: Neoadjuvant therapy is the first treatment for breast cancer, given before surgery.17
- Recurrence (Relapse): A recurrence or relapse means that the cancer has returned, usually after a period of time during which the cancer could not be detected. The cancer may come back to the same place as the original (primary) tumor or to another place in the body.17,24
Understanding HR+, HER2- breast cancer can help people living with breast cancer and their loved ones feel more informed as they navigate diagnosis and treatment. While every person’s experience with cancer is different, there are a range of treatment options available that can be tailored to each individual’s diagnosis and needs. It’s important for patients to speak with their healthcare team to better understand their specific cancer and what treatment approach may be right for them. Advances in research continue to improve how HR+ breast cancers are treated, with expanded options that can potentially achieve even better outcomes over time.